
Microdosers it was more likely that no microdosers be older (Xtwo (2, N = 1133) = 22.13, p < 0.01), white ethnicity (Xtwo (1, N = 1133) = 4.62, p = 0.03) and to report full-time employment (Xtwo (3, N = 1122) = 11.83, p<0.01); groups were equivalent in all other demographic domains (all Xtwo‘s < 6.03, all P.S. > 0.05; See table 1). Comparisons between dose microdosers and microdosing days in the past month found no differences between Years (days: Xtwo (2, N = 953) = 3.37, p = 0.19; dose: Xtwo (2, N = 953) = 3.31, p = 0.19) and mental health concerns (days: Xtwo (2, N = 931) = 0.71, p = 0.70; dose: Xtwo (2, N = 931) = 0.21, p = 0.90).
Preliminary analyzes identified the expected differences according to Years ; the group under 55 years of age demonstrated superior performance to the group over 55 years of age in all cognitive tasks; for Tap Test (Mean = 70.48 (33.18) versus 52.60 (29.99); you (1, 863) = 5.05, p <0.01); for PASAT (Mean = 33.67 (14.21) vs. 30.37 (12.92) you(1, 772) = 2.08, p <0.05) and spatial amplitude (mean = 236.25 (51.02) vs. 176.88 (58.80); you (1, 943) = 11.00, p<0.01). Baseline differences by Years they were identified by negative mood (mean = 46.89 (16.13) versus 40.64 (16.06); you (1, 1048) = 3.96, p <0.01) but not positive mood (mean = 55% (16) vs. 55.03% (15.01); you (1, 1048) = − 0.018, p = 0.99). As expected, the participants who reported mental health concerns showed higher scores on all three DASS subscales: depression (mean = 10.44 (9.72) vs. 18.92 (12); you (1, 1010) = −11.81, p <0.01); Anxiety (mean = 6.38 (6.36) versus 11.38 (8.74); you (1, 1010) = 10.09, p < 0.01) and Stress (mean = 13.84 (9.1) vs. 20.04 (9.8); you (1, 1010) = 9.61, p <0.01). Gender analysis revealed no main effect of gender over time in any of the DASS domains (All F < 1.6, p > 0.20).
Depression, anxiety, stress
Comparisons of microdosers with non-microdosers in change from baseline to month-1 (Microdose*time ) indicated greater improvements between microdosers in the DASS domains of Depression (F (1, 1019) = 17.91, b = 0. 12p <0.01), Anxiety (F (1, 1017) = 18.33, b = 0.08p <0.01), and Stress (F (1, 1016) = 15.60, b = 0.08p <0.01) (fig. 1; Table two). These effects remained consistent after removal of 124, 82, and 75 outliers within anxiety depression, Y Stress domains respectively for scores exceeding 2 standard deviations from the mean (all Microdose*time F > 7.99 p <0.01), and in parallel analyzes restricted to the 594 participants who did not report microdosing before baseline (all Microdose*time F > 4.17, p <0.05). We identify a Microdose*Gender*Time interaction such that the effect of microdosing over time was found to be moderated by gender in DASS depression. Specifically, microdose-related reductions in depression were stronger among women than men (F (1, 1016) = 6.61, b = 0.17p = 0.01). Nope Microdose* Gender*Time interaction was identified for DASS anxiety (F (1, 1024) = 1.14, b = 0.46, p = 0.29) or DASS stress(F(1, 1023) = 0.90, b= 0.05, p= 0.34).
The interactions between Mental health concerns and microdosing groups were not significant for any of the domains (all Microdoses*Mental health problems*TimeFs < 1.16; p> 0.10), indicating that the main effects of microdosing were consistent between respondents with and without mental health problems. Among the microdosers with mental health concerns,scores in depression changed from 18.85 (12.03) at baseline to 11.73 (9.85) at Month-1; by anxiety, 11.04 (8.48) at baseline to 7.46 (6.68) at Month-1; and to stress,19.93 (9.71) at baseline to 13.91 (9.02) at Month-1. Among respondents with no history of mental health concerns, scores in depression changed from 10.40 (9.78) at baseline to 6.65 (7.60) at Month-1; by anxiety,6.53 (6.50) at baseline to 4.81 (5.57) at Month-1; and to stress, 13.96 (9.12) at baseline to 9.78 (7.50) at Month-1. Supplementary analyzes compared stacking conditions on changes in DASS depression, anxiety, and stress scores from baseline to month 1. No difference between Psilocybin Microdosers OnlyY psilocybin + HE Microdosers (allF<0.70; p > 0.10) were observed. Likewise, there are no differences between Psilocybin Microdosers Only Y psilocybin + THE +B3 microdosersthey were identified (everybodyF<0.77; p> 0.10 ).
Mood
Findings on both subscales of the PANAS mirrored those of the DASS. Relative to no microdosers, microdosersexhibited greater increases in positive mood from baseline to month-1 (F(1, 1058) = 59.98,b= −0.32,p< 0.01) and greater decreases in negative mood over the duration of the study (F(1, 1059) = 33.76, b= 0.23p<0.01). These effects remained consistent after removal of 75 and 76 outlier responses within the positive and negative mood domains, respectively, for scores that exceeded two standard deviations above or below the mean ( all Microdose*timeF > 26.32;p< 0.01), and among the 479 participants microdosing at the time of study entry ( all Microdose*timeF > 22.05;p<0.01). Furthermore, moderating analyzes indicated that these effects were stable across genders ( all Microdose*Gender*TimeF<1.94; p> 0.05).
The interaction between age, microdosing status, and time was not significant for positive mood (F(1, 1058) = 0.21, b= − 0.05, p= 0.65) or negative mood ( F(1, 1059) = 1.38, b= 0.13 p= 0.24), indicating equivalence of mood effects across age. Follow-up analyzes identified no significant differences in changes in positive or negative mood over time between Psilocybin Microdosers Onlyand either the psilocybin+ HE microdosers(all F < 0.52, p> 0.47) or the psilocybin+THE+ B3 microdosers(all F < 2.44, p> 0.12).
Psychomotor performance and cognition
Analyzes of the finger-touch test identified a main effect of microdosing, so thatmicrodosersdemonstrated a more positive change in performance than non-microdosers (F(1, 886) = 9.09,b= −0.24,p= 0.03 ;Table two). Supplementary analyzes revealed no significant 3-way interaction betweenMicrodose, Gender and Time,indicating that the effects of microdosing were consistentGender(F= 0.26 b= 0.94,p= 0.61). The effect of microdosing on touch score over time was robust to the elimination of 16 outlier responses with scores 2 standard deviations from the mean (Microdose*Time F= 7 .23 b= −0.21,p= 0.07), and treatment effects were held constant when the study sample was limited to the 515 participants who were not microdosing at baseline (Microdose*Time F= 5.07b= 0.22,p= 0.03). Finally, the interaction betweenMicrodose* Time*Agewas not significant ( F= 3 .41 b= 0 .43 p= 0 .06), indicating that the effect of microdosing was constant at all ages.
Stacking analysis between microdosers (Fig. two) found no interaction ofPsilocybin alone versus psilocybin+ Time,suggesting that the addition of HE did not affect the effect of psilocybin on finger touch (F(1, 524) = 0.284,b= 0.12, p= 0.67). On the contrary, thePsilocybin alone vs psilocybin+THE+ B3*Timeinteraction indicated a relatively greater improvement in tap scores with the addition of HE and B3 to psilocybin (F(1, 732) = 3.93, b= −0.51,p< 0 .05). This finding was followed up by examination of the moderating effect of age, which identified aPsilocybin alone vs psilocybin+ THE+B3 * Time*Yearsinteraction (F(1, 732) = 8.4, b= 0.6 p= 0 .04), which reflected that the addition of HE and B3 had an impact among older respondents but not among younger respondents. Complementary analyzes of psilocybin+ HE vs psilocybin+ THE+ B3 * Timerevealed a trend towards significance (F(1, 427) = 3.26, b= −0.56 p= 0.07), and triplepsilocybin+HE vs psilocybin+THE+B3 * Time*Yearsinteraction was identified (F (1, 427) = 6.71,b= 0.66p= 0.01), indicating that the effects were more pronounced among older respondents. Follow-up supplemental analyzes indicated that these findings were robust after controlling for subgroup differences in age, microdose frequency, and microdose dose (all 3-way interactions Fs > 6.20,p<0.05).
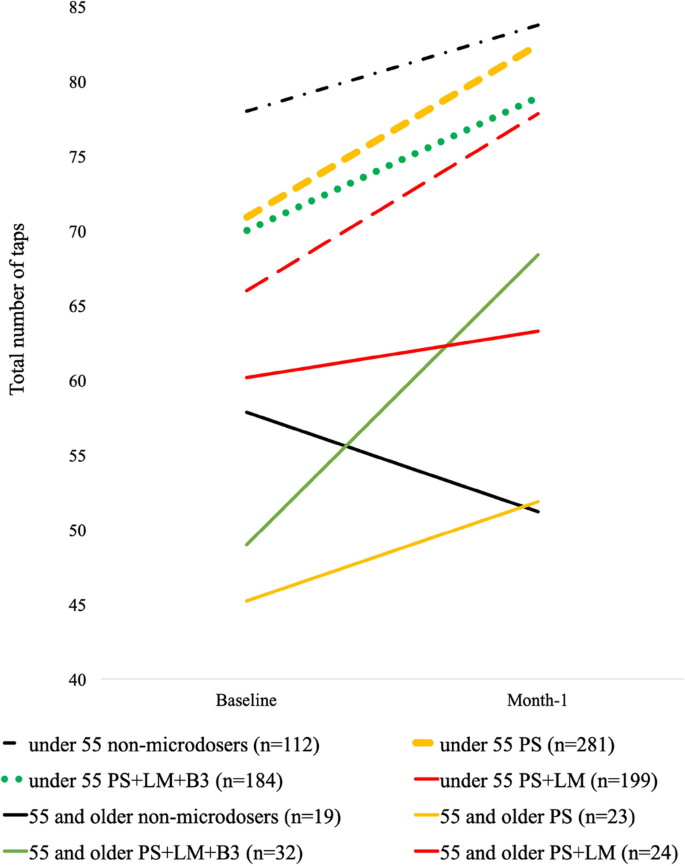
Microdosing and Finger Touch Test Scores. The “baseline” values reflect the mean responses of the participants collected from 0 to 7 days from the start of the study. “Month 1” values reflect mean participant responses collected between 22 and 35 days after the start of the study. PS refers to participants who microdosed psilocybin in the absence of Lion’s Mane (HE). PS + HE refers to participants microdosing with psilocybin and HE in the absence of niacin (B3). PS + HE + B3 microdosers refer to participants who microdosed psilocybin with HE and B3. The differences in the slopes of group condition were subjected to Microdose*Time interaction analysis.
comparisons ofmicrodosersano microdosersin the change from baseline to month 1 indicated no difference for thespatial amplitude task(F(1, 944) = 0.24,b= −0.07,p= 0.63) or thePASAT(F(1, 775) = 0.21,b= 0.02,p= 0.65). In light of this lack of main effects, no follow-up analyzes were performed.